
My first exposure to computers was at age
6 (1963), as a subject in Dr.
Patrick Suppes' accelerated mathematics experiment at Stanford. I was
taken to a small room with what I now know was a CRT display and an intercom.
I was asked to push some keys in response to some shapes on the screen. Afterwards,
they showed me around a large room filled with big cabinets, some with lots
of blinking white lights.
They said it was a "computer" and its name was
the "PDP-1". A tall thin
man asked me to hit a key on a console to make a "decktape". I had absolutely
no idea what a "DEC tape" was at the time, but when I hit the key, a small
pair of reels BEGAN TO TURN!! It was a moment I would never forget.
By age 10 I began constructing all kinds of
electronic hobby projects, and had also done some soldering of "Flip Flop" boards (with my
cousin) for a friend of his father's named Burt Libe (Some of these boards
wound up as part of a "sound tree" exhibit which is still in operation at
the Exploratorium in San Francisco.  A visitor would clap his hands or speak,
and a colorful wave of light would sweep up the tree.) I also built model
rockets (this was still the age of Apollo) and through that hobby learned
of Micro Instrumentation and Telemetry Systems: MITS (they were selling flashing
light kits for night launches of model rockets, but no Altair computer yet.)
A visitor would clap his hands or speak,
and a colorful wave of light would sweep up the tree.) I also built model
rockets (this was still the age of Apollo) and through that hobby learned
of Micro Instrumentation and Telemetry Systems: MITS (they were selling flashing
light kits for night launches of model rockets, but no Altair computer yet.)
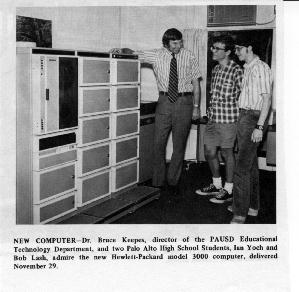
Back in 1973 I was an energetic Palo Alto
High School student who had recently become a student System Operator for
the PAUSD school district's HP2000F 32-user BASIC timeshare computer system
(under the direction of Dr. Bruce Keepes), which was later upgraded to a
prototype HP3000.
The HP2000F had a bank of 110 BAUD modems (10
characters per second) for teletype dial-ups, as well as "Fast Ports" at
300 BAUD. One afternoon I was at the People's Computer Center and
used one of their ASR 33 teletypes with an acoustical coupler
(you actually put the telephone handset into a cradle on the slanted face
of the teletype) , dialed in, and had an online "chat" with fellow HP2000F
system operator Greg Dolkas (who later went on to work at HP, I understand).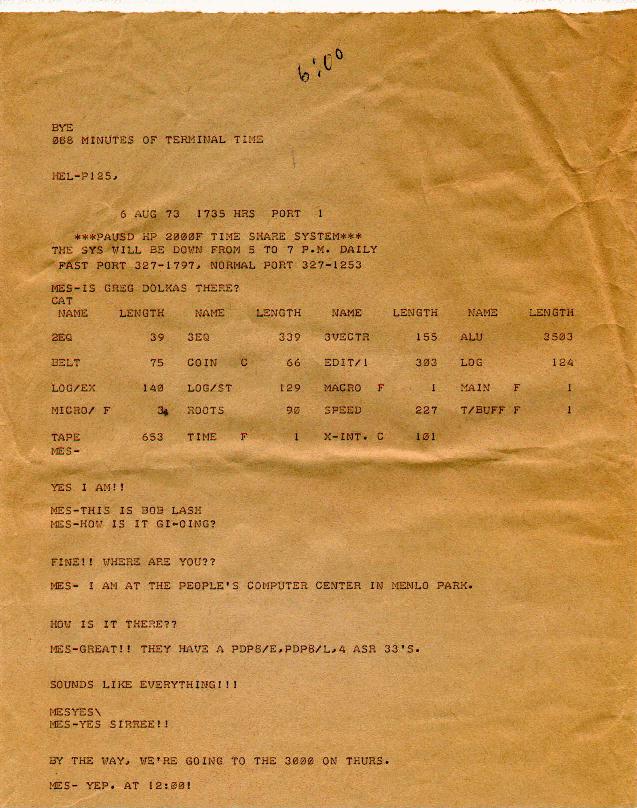
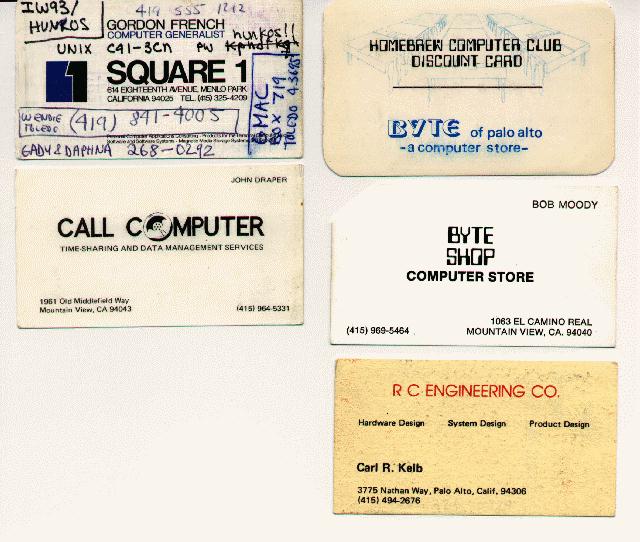
The People's Computer Center was a really cool place for computer hobbyists at that time -- as you see in the printout, they had a PDP-8/E, PDP-8/L, and 4 ASR 33 teletypes... the best public access for "real people"!
Posted on a bulletin board in the PALY terminal room (containing 6 noisy KSR-33 teletypes in the Palo Alto High School math-science office) was a notice that a computer group meeting would be held at the home of Gordon French. Mike Fremont (another student System Operator) and I both attended this first meeting of the Homebrew Computer Club in Gordon French's garage. We were the two youngest ones there, and rather shy and quiet, but were absolutely astounded when Gordon let us step into his house and see his 8008 system using 16K of SHIFT REGISTERS (!) as memory and his very own teletype (unlike random- access memory, his system actually shifted the data in a ring and WAITED until the desired address came up for data read/writes! We were extremely impressed.).
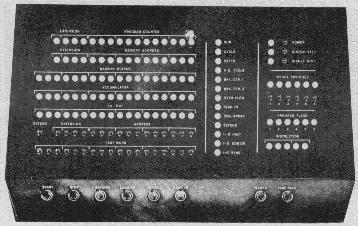
 The excitement at homebrew was electric, and
during the period of '74 to '76 I constructed a working 12-bit microprogrammed
minicomputer (see photo) using a 30-bit micro-control store entirely
out of about 100 SSI/MSI TTL wire-wrapped chips, which (thanks to the understanding
of my wife) I still have. My cousin often sat in the freezing garage with
me late at night helping with the wire-wrapping. No microprocessor chip was
used initially because as a kid, using 4004's or an 8008 was prohibitively
expensive. (I was working as a "soda jerk" at Edy's across the street from
the Stanford Campus along with three lawn mowing jobs to pay for parts. One
night, after returning home from Larry Page's with a tiny little bag of 256
bit (BIT, not K) ram chips my mother, in a shocked tone, said "That's what
your month's pay went into??!!" ). The front panel has about 100 incandescent
lamps (Gordon thought these were especially neat when he came over for a
demonstration) and 56 toggle switches. It was hooked to an ASR-33 which I
reconstructed from 3 junked teletype chassis given to me by a friend, David
Bell. (This was a BIG improvement over the Model 17 teletype he pawned off
on me earlier, which while indestructible, dimmed the lights in my garage,
leaked blue sparks from its typing distributor, suffered from the handicap
of 5 bit BAUDOT code instead of ASCII, and apparently was taken out of service
by a newswire service in the 1930's.)
The excitement at homebrew was electric, and
during the period of '74 to '76 I constructed a working 12-bit microprogrammed
minicomputer (see photo) using a 30-bit micro-control store entirely
out of about 100 SSI/MSI TTL wire-wrapped chips, which (thanks to the understanding
of my wife) I still have. My cousin often sat in the freezing garage with
me late at night helping with the wire-wrapping. No microprocessor chip was
used initially because as a kid, using 4004's or an 8008 was prohibitively
expensive. (I was working as a "soda jerk" at Edy's across the street from
the Stanford Campus along with three lawn mowing jobs to pay for parts. One
night, after returning home from Larry Page's with a tiny little bag of 256
bit (BIT, not K) ram chips my mother, in a shocked tone, said "That's what
your month's pay went into??!!" ). The front panel has about 100 incandescent
lamps (Gordon thought these were especially neat when he came over for a
demonstration) and 56 toggle switches. It was hooked to an ASR-33 which I
reconstructed from 3 junked teletype chassis given to me by a friend, David
Bell. (This was a BIG improvement over the Model 17 teletype he pawned off
on me earlier, which while indestructible, dimmed the lights in my garage,
leaked blue sparks from its typing distributor, suffered from the handicap
of 5 bit BAUDOT code instead of ASCII, and apparently was taken out of service
by a newswire service in the 1930's.)
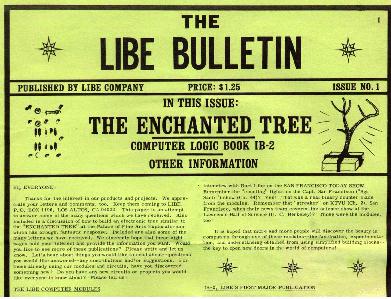
Gordon French recently reconnected with me (thanks to the Net!), and I was amazed to learn he technically still holds the position of Secretary of Homebrew! He is in the process of collecting up some of the early notes and newsletters for scanning, and sent me this page (click on excerpt below) from his notes about the meeting... it also announces that our next meeting would be held at Peninsula School:
Gordon is also still active as the Chairman of a model engine builder's group.
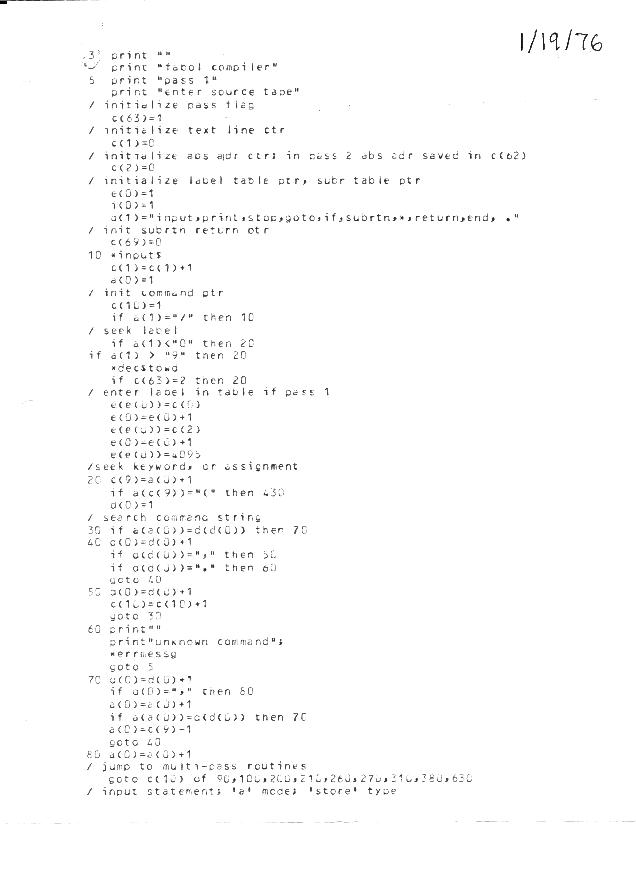
Remember those paper tapes? Well, with the
right incantations, the ASR-33's balky paper tape reader could usually be
coaxed to load the bootstrap: 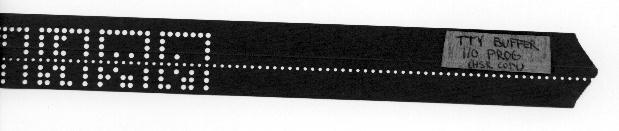 I wrote an assembler and compiler for it. The compiler was called FABOL, for "Fortan-Assemby-Basic
Oriented Language". I later donated the Burroughs tape drive (which I inherited
from homebrewer Carl Kelb
- RC Engineering) to the Foothill College Electronics Museum.
I wrote an assembler and compiler for it. The compiler was called FABOL, for "Fortan-Assemby-Basic
Oriented Language". I later donated the Burroughs tape drive (which I inherited
from homebrewer Carl Kelb
- RC Engineering) to the Foothill College Electronics Museum.
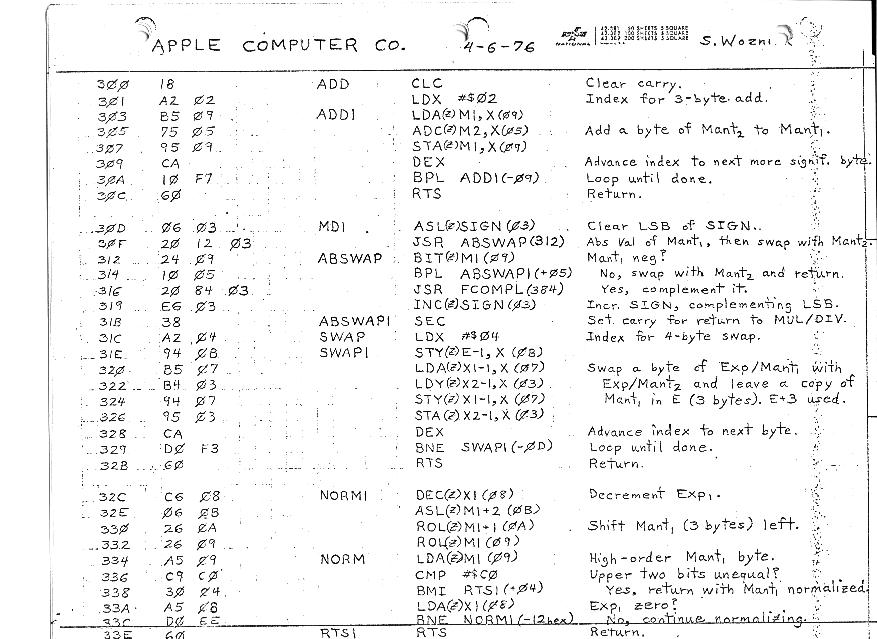
In 1976 Steve Wozniac gave me a copy
of his 6502 floating point math
routines which I laboriously typed byte-by-byte onto paper tape late
into the night. I had by then added a 6502 chip to my system to function
as its floating point processor(!). The thrill of actually seeing it all
work was indescribable.
While in High School, I landed a summer Engineering Internship at the Stanford Linear Accelerator Center (SLAC), where I successfully constructed an embedded controller for a hydrogen target experiment.
I later did an Engineering Internship at IBM, where I helped to develop a real-time motion controller for an open-reel magnetic tape drive. This was extremely fun, especially when minor bugs sometimes filled the lab ankle-deep with magnetic tape! I learned a great deal about how to use Programmable Gate Arrays for high performance motion control that summer.
My father, Harvey Lash, M.D., D.D.S., (founder of the Department of Plastic Surgery at the Palo Alto Medical Clinic, and a clinical professor at Stanford) used to "test out" his slide talks on me while I was growing up, and I was constantly amazed by what I saw. My father invented the first prosthetic penile implant to correct impotency in males (the Lash Penile Implant, produced by Dow Corning in the 1960's), developed an artificial tooth implant, and pioneered the very first use of the Argon laser to remove "port wine stain" hemangioma birthmarks (like the one on Gorbachev's forehead).
While still in High School, I concluded that while computers and electronics were incredibly fun, they were not ends-in-themselves. I wanted to help make the world a better place. So, I decided to dedicate my career to applying engineering to medicine. I also decided I would do this by first getting an engineering degree, then becoming an M.D. (to learn the application area, but not to practice), and then forming a medical device development company.
So I earned my B.S. in Electrical Engineering
and Computer Science at U.C. Berkeley, and was in the School of
Engineering's Bioelectronics concentration program. I earned "A+" grades
in many of my biomedical electronics courses because I especially loved those
subjects.
 I created my first medical device while in college
in 1978: a surgical nerve stimulator. Stanford Hospital needed to
replace one of their surgical nerve stimulators (used to identify and isolate
nerves during surgery), but the manufacturer of their favorite model had
gone out of business! My father asked if I could develop a new unit
with equivalent features, and I eagerly jumped at the chance! My first
"big break" !!
I created my first medical device while in college
in 1978: a surgical nerve stimulator. Stanford Hospital needed to
replace one of their surgical nerve stimulators (used to identify and isolate
nerves during surgery), but the manufacturer of their favorite model had
gone out of business! My father asked if I could develop a new unit
with equivalent features, and I eagerly jumped at the chance! My first
"big break" !!
The old unit's circuitry was potted in a
block of epoxy, so there was no way to know the design they used. However,
I carefully measured the output characteristics of one of their remaining
units using a scope and test loads, and designed my own circuitry to precisely
replicate the signals and output impedance levels. I also constructed sets
of bipolar electrode probes using molded acrylic, which were ETO sterilized.
The surgeons loved the new unit!
The next year I designed and constructed microprocessor-based
fully automated hearing tester for a biomedical instrument course.
The system worked beautifully, and could be
run by the layman. No audiologist was required. The system generated a series
of calibrated test tones over a range of frequencies and dB power levels,
and the patients simply pushed a button each time they could hear a tone
in their headphones. The system printed a final hardcopy audiogram. It was
cool!
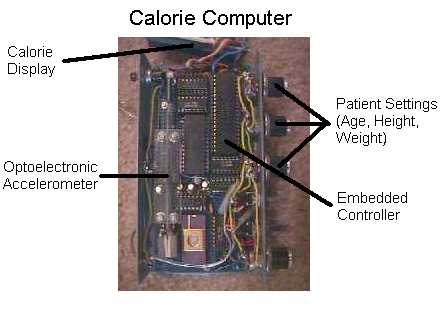 Another medical device I created while still
in college was the "Calorie Computer." This device clips to
your belt, and reports the number of calories you have burned in real-time
based on your actual activity. I devised a low-cost accelerometer using an
optical beam passing through a photogradient mask. The mast was affixed to
a spring-loaded weighted acrylic plate, which moved up and down with each
step taken by the subject. My code analyzed the waveform collected
by the analog-to-digital converter using real-time Digital Signal Processing
techniques, and was able to determine whether the subject was walking, running,
jogging, or at rest. Then, using the patient's settings for Age, Height,
and Weight, I computed their resting basal metabolic rate, and then added
the calories burned due to activity on top of that, resulting in total calories
burned being displayed.
Another medical device I created while still
in college was the "Calorie Computer." This device clips to
your belt, and reports the number of calories you have burned in real-time
based on your actual activity. I devised a low-cost accelerometer using an
optical beam passing through a photogradient mask. The mast was affixed to
a spring-loaded weighted acrylic plate, which moved up and down with each
step taken by the subject. My code analyzed the waveform collected
by the analog-to-digital converter using real-time Digital Signal Processing
techniques, and was able to determine whether the subject was walking, running,
jogging, or at rest. Then, using the patient's settings for Age, Height,
and Weight, I computed their resting basal metabolic rate, and then added
the calories burned due to activity on top of that, resulting in total calories
burned being displayed.
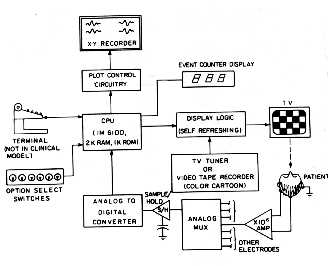 During my last 2 years in college I designed
and constructed a working microprocessor-based Visual Evoked Potential
(VEP) measurement system which can be used to objectively measure
visual acuity in infants, as well aid in the early diagnosis of multiple
sclerosis. I worked under Dr. Elwin Marg, who was a professor at U.C. Berkeley's
School of Optometry. My device displayed a set of repetitive visual
stimulus patterns on a TV screen, and time-averaged the patient's EEG. Any
part of the EEG that was not related to the visual stimulus averaged out
to zero, leaving behind a characteristic waveform that corresponds to the
visual signal being conducted from the retina down the optic nerve to the
visual cortex.
During my last 2 years in college I designed
and constructed a working microprocessor-based Visual Evoked Potential
(VEP) measurement system which can be used to objectively measure
visual acuity in infants, as well aid in the early diagnosis of multiple
sclerosis. I worked under Dr. Elwin Marg, who was a professor at U.C. Berkeley's
School of Optometry. My device displayed a set of repetitive visual
stimulus patterns on a TV screen, and time-averaged the patient's EEG. Any
part of the EEG that was not related to the visual stimulus averaged out
to zero, leaving behind a characteristic waveform that corresponds to the
visual signal being conducted from the retina down the optic nerve to the
visual cortex.
This method can determine how well infants can see to within 1 diopter.
In the case of multiple sclerosis this method
reveals a "stretching out" of the waveform beyond normal, due to slowed nerve
conduction.
When I applied to medical schools, I told them up-front that I had no intention of ever practicing, and only wanted to develop medical devices. I was afraid this would count against me, but in fact the schools thought my plan was great, especially as they were facing an oversupply of clinicians at the time!
I was accepted into my first choice of med schools... U.C. San Diego. Not only do they have an excellent engineering program there, they permit each medical student to do an independent doctoral thesis project. So, I decided to design an algorithm that would allow paraplegics to walk again with independent balance, using a proposed implantable system.

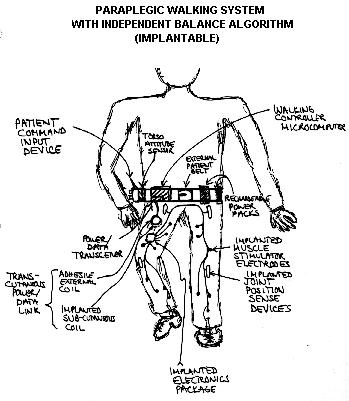
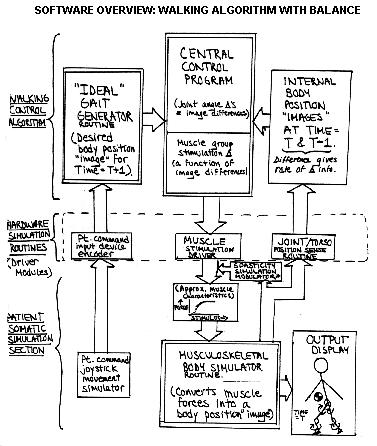
The key to independent balance was my inclusion
of an externally worn "torso attitude sensor" (inclinometer) to replace the
inner ear's balance feedback mechanism. To test the algorithm, I simulated
both the implantable hardware and the patient's musculoskeletal biomechanical
system using sophisticated computer modeling techniques (my musculoskeletal
model factored in the actual origin and insertion locations of 28 muscle groups
in the lower extremities, along with muscular response to stimulus, time
lags, length-tension effects, isometric contraction behavior for each, gravitational
and muscular torques, inertia about joints, and centroid gravitational centers).
I transformed the algorithm into running code, and successfully tested it
against the simulated paraplegic patient... and after solving some head-over-heels
falling problems, the simulated patient walked! This field is still
in its infancy, and we are going to see many exciting advances in the years
ahead.
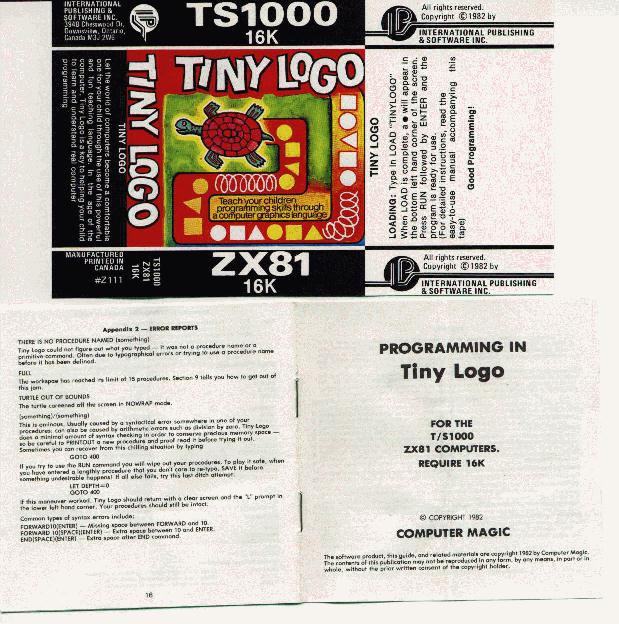
In '82 I wrote a TINY LOGO interpreter to help open up the world of programming to children. My software was published by a Canadian based software house for the ill-fated TIMEX/SINCLAIR computer. I thought that this $49 computer that could run BASIC would really be a hit, but it became clear that the average buyer wasn't really interested in programming at all. (I took some inspiration from Tom Pittman who wrote TINY BASIC back in homebrew, and demonstrated that you could run a nice little interpreter in a tiny amount of program space).
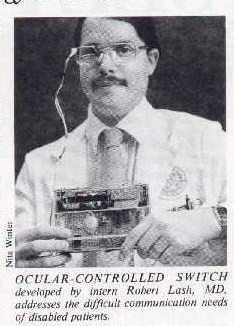
I then developed a device to allow quadriplegics to type out messages via eye-blink, and summon nursing help on demand. There was a patient on my service with high quadriplegia secondary to basilar artery thrombosis, and I knew I could help, so I built it for him. My ocular controlled switch works by bouncing a beam of infrared light off of the patient's eye, which is then picked up by a photodetector mounted into an eyeglass frame. When my system's electronics were connected to a scanning alphabet board and printer, the patient was able to communicate.
After receiving my M.D. degree from U.C. San Diego, I decided to do my internship at St. Mary's Hospital in San Francisco in order to learn first hand how medical devices were really being used on the floor and in the operating room. It was a fascinating year. For example, engineers tend to be conservative when setting alarm limit parameters, and so when frequent false alarms occurred (such as I saw in some IV pumps, for example), the nurses just switched the speaker off and ignored the alarms completely. I carried these kinds of practical lessons with me as I later moved even deeper into medical device work.
During internship I met another Intern who was also an engineer, and we decided to start a medical device venture called M.D. Engineering, Inc.. In 1984 we came up with a list of 30 entirely novel medical devices (using market gap analysis) and then chose the top ones to pursue initially. We raised $2 million in seed capital from private investors (the co-chairmen of Consolidated Capital) .
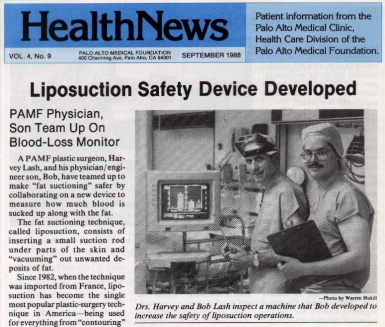
Liposuction was becoming popular, and my father (who had been examining the procedure) alerted me to some cases of unexpected hypovolemic shock due to blood loss. When you "suck out the fat" you also can damage small vessels and "suck out the blood", but it is difficult to tell how much blood is in the collected fat / blood mixture. Also, to help achieve a more symmetrical result, it would be extremely useful to know how many cc's of pure fat was removed from each area.
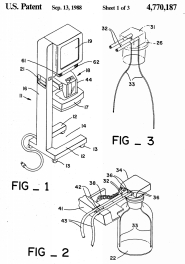
So I created a Liposuction Blood Loss Monitor
(the "LM2000"). It occurred to me that blood is an excellent electrical
conductor (due to dissolved electrolytes) and that fat is an excellent insulator
(being a non-polar lipid). I confirmed via in-vitro experiments that by measuring
the electrical impedance of the collecting jar with a pair of electrodes,
the ratio of fat-to-blood could be determined. Then by weighing the jar with
an electronic load cell and multiplying the ratio, the number of cc's of
fat and blood could be accurately determined. This microprocessor-based
system also displayed cc's of pure fat removed by area, and featured a transfusion
limit alarm.
M.D. Engineering continued to grow, and became the largest producer of Liposuction equipment at that time (the company was later acquired by Medical Device Resource Corporation, which continues to produce many of these products today). I was CEO, and also headed up R&D. We were the "big fish in a small pond" with 10 full-time employees, 10 part-time consultants, and my VP of Sales led 70 independent sales reps for us (he was formerly the Western Regional sales manager for American Hospital Supply Corporation).
To speed up the liposuction procedure (and
reduce O.R. time and patient anesthesia risk), I developed a high performance
surgical aspirator (the "LS1000" - see below). Every time surgeons
were inserting a liposuction cannula, they were typically waiting 12 seconds
or longer until the fat started to flow. It occured to me that by doubling
the airflow rate, the air in the collecting jar could be evacuated twice
as fast, achieving full vacuum in half the time. Tests confirmed that the
design cut the waiting time down 50%. We caught our competitors by
surprise, and these units started "selling like hotcakes."


More add-on Liposuction products were developed quickly, and I oversaw the development of an implosion-proof disposable collecting canister, a high-flow anti-pathogen filter, a full line of cannulae, sterile tubing, post-surgical compression garments, and fat micrografting systems.
Then one day, the head of Sales walked in to my office and said "we need a Laparoscopic Insufflator!" I said, "O.K.., we can do it.... how come?" He had a struck a deal with Snowden-Pencer (a manufacturer and distributor of mechanical laparoscopic hand instruments) under which we would design and manufacture a High Flow Laparoscopic Insufflator for them under an OEM private label deal. These units keep the abdomen inflated with C02 gas as minimally-invasive surgery is conducted through small openings.
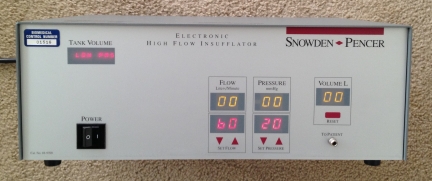
This was an exciting product, and under my direction our team created the highest performance Insufflator ever produced at the time. We used an embedded control scheme involving solid-state pressure transducers which could tightly control both flow and pressure using pulse-width-modulated solenoid valves. By doubling the flow rate over competing products, our unit quickly responded to sudden losses of abdominal pressure (which can happen due to trocar area leaks, or aggressive smoke suctioning) and could prevent catastrophic loss of pneumoperitoneum better than the competitors. The product sold well.
Then, the head of sales walked in and said "now we need a Cold Fiberoptic 300 Watt Xenon Lightsource with an auto-iris!" It was another Snowden-Pencer deal. I said "O.K., we can do it!" These products supply cold white light to endoscopes (via fiberoptic cables) to light up the inside of the patient. To maintain a steady lighting level for the endoscopic camera, I designed circuitry to strip off the NTSC video luminance levels, and integrated these to drive a DC servomotor that controlled the light output by turning a variable aperture disk. It was a great device.
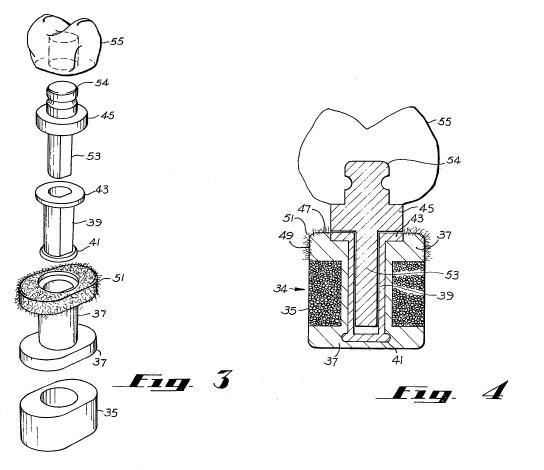
I should also mention the Lash Oral Implant. This unique artificial tooth was patented by my father, Harvey Lash, M.D., D.D.S., and provided to my company for further development. The first design involved a porous ceramic which allowed the bone of the jaw to grow into the socket, and a silicone shock absorber to extend the implant longevity. A dacron lip permitted the gum to grow into the surface of the socket, thereby sealing it. The crown and pin was then inserted into the socket. Animal studies and preliminary human tests were conducted, and the device worked. An improved porous titanium socket was designed. Unfortunately an expected grant for further trials did not materialize.
There are two more devices I invented at M.D. Engineering that deserve mention, both of which were on the "original list of 30 devices."
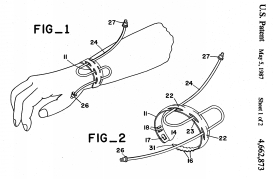
I noticed in the hospital that I.V. lines sometimes would snag and get pulled out. Why not create an I.V. Tube Stress-relief Bracelet ? So I cut slots into a wrist band (similar to the plastic I.D. band placed around a patient's wrist upon admission), loosely adjusted it (with two finger-widths of wrist space as done for an I.D. band in case of unexpected swelling), threaded a piece of IV extension tubing through it, and was delighted to see that I could give the tube up to a 40 pound yank without disturbing the IV needle site. What a great idea! We contacted Becton-Dickinson, and they got very excited, saying they could see placing a roll of these on every floor cart in the world. So we organized some focus groups (consisting of floor nurses), and were shocked to discover that even though they routinely apply plastic I.D. wrist bands, they would not use this device because it broke their nursing rule that "nothing must encircle the wrist." Even though this could even be implemented by actually putting slots *in the ID wrist band*, we were unable to overcome their rigid adherence to this policy.
The other device I wanted to mention was the "Smokeless Low-Noise Electrosurgical Scalpel." I noticed that in operations where electrosurgical scalpels were used (for cutting and coagulation), the staff wound up inhaling lots of smoke. What they wanted was a smoke evacuation system that would be both effective and very quiet. I realized the problem of high flow with low sound emission could be solved by applied fluid dynamics, so I engaged an aerospace consulting firm (they had done turbulence sound reduction work for the Navy under a Trident Submarine contract) to help with the prototyping. A clever "silencer" scheme was used which allowed for fast flow, yet prevented the sound from escaping. However, in animal tissue tests we discovered that the high airflow caused some distortion of the electrocautery's spark-discharge paths. More R&D budget would be needed to resolve that issue, and I made the business decision to back-burner the project.
At that time AIDS was on the rise, and one
afternoon my father, Harvey Lash, M.D., who as I mentioned earlier invented
the original silicone rod penile implant to correct impotency, sketched out
his concept for a female condom on the back of an envelope, and wanted
to know if I could develop it. What a terrific idea! He assigned
his patent rights to M.D. Engineering, and I began prototyping work immediately.
So in 1989, with working prototypes in hand,
I brought in funding from Hambrecht and Quist and we formed a spin-off company
called M.D. Personal Products to develop the female condom.
I left M.D. Engineering to become Vice Chairman and Chief of Research and
Development. I also acted as the interim CEO, until we were able
to recruit a former VP of Marketing from Kimberly-Clark named Tom Hatch.
Tom had invented the panty-liner pad while he was at Kimberly-Clark, and
was an expert in intimate consumer products for women.

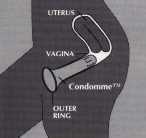
The "Women's Choice Female Condom" is a latex vaginal liner that is inserted with a tampon-like applicator. The thickened pleated latex tip slenderizes during insertion and then pops open like an umbrella, providing enough traction in the upper vagina to prevent the liner from accidentally slipping out. An external ring keeps the device open, and can be easily grasped for removal.
We successfully completed the first two phases of FDA clinical studies, and things were going very well. Then, a women's group in Washington sent a protest to the FDA, saying the agency should not consider female condoms to be substantially equivalent to male condoms, but rather should compare them to birth control pills. The FDA agreed, and reclassified female condoms from Class II to Class III. Suddenly we needed to conduct at least two more years of clinical trials, which would cost millions more. Hambrecht and Quist was not prepared to come back in to cover the new cost. I contacted many V.C.'s, but most all (understandably) asked the same question: "Why isn't H&Q coming back in to take the lead?" We were unable to raise the needed round, so I had to let the entire staff go.
Around that time, my wife was in a company that was to become WebChat, and they needed my software development and entrepreneurial management skills, so I joined them (this is how I got swept into the "dot com" world). We created the first chat system for the Web, which we grew from 5 users to 3 million users, and we were running the largest community on the web when we were acquired by Infoseek. As Chief Technology Officer for WebChat, I was the principal architect for our massively scalable server farm, and managed our software engineers and 24X7 IT services. Disney then acquired Infoseek, and I oversaw WebChat's integration into Disney's GO.com, ESPN.com, and ABC.com properties.
Then in 1998 the founder WebChat, Mike Fremont, formed a "dot com" called Zorch, Inc. and a group of "WebChat Alumni", including myself, left Disney's GO.com to join him there. I became Chief Technology Officer, and led the development of a massively scalable educational online service for kids. We created a wonderful site for kids as young as 7 build, learn, and even create their own programs, but unfortunately the venture capital pendulum swung away from community and towards business-to-business investments. We were unable to raise our next round.
In 2000 I was recruited to become VP of Engineering for Driving Media, which was founded by Dave Morse. Dave also founded Amiga Computer, 3DO, and Crystal Dynamics. I hired and managed our software engineering and IT teams, and led the development for a massively scalable automotive portal for consumers. Unfortunately the "dot com bubble" burst completely at that point, and the company could not raise its next round, so the staff had to be laid off.
I then looked at various opportunities, but concluded that the dot com sector was not likely to regain its vitality any time soon. I decided that I wanted to "return to my roots" of medical device development.
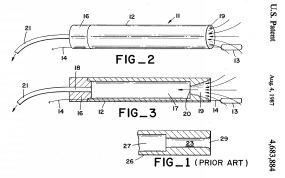
By the way, I kept my hand in medical device
development even during the time I was in the dot com world! A friend
of mine, Sean Maloney, M.D., is a rehab medicine specialist, and we have successfully
developed a device to allow quadriplegics to control their PC's using tongue
movements in place of a mouse, which we call the Intraoral Controller:
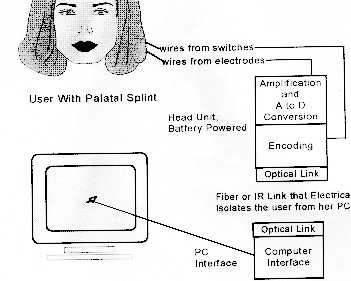

We obtained NIH grants (winning SBIR Phase I and Phase II awards) for the project, and I handled the electrical engineering design and digital signal processing software work. The device consists of a palatal splint (similar to a dental retainer plate) that clips to the roof of the patient's mouth. It contains embedded surface EMG electrodes which sense the X-Y movement of the tongue. The beauty of this design is that unlike mouth operated mechanical joysticks, the patient can freely speak and swallow while it is in use.
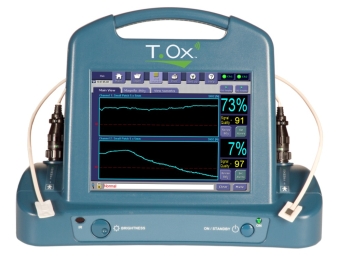
In 2002, I became VP of Engineering at ViOptix (and in 2008 Sr. VP and Chief R&D Officer) where I led the development of a Tissue Oximeter. This is a non-invasive system consisting of a touchscreen driven console and a variety of sterile disposable fiberoptic based sensors to measure tissue oxygen saturation and tissue hemoglobin. The console features Wi-Fi transmission to a backend Linux server farm to allow remote viewing of readings on an iPhone, Blackberry, Android, or web browser. Applications include plastic surgery, shock, peripheral vascular disease, spinal surgery, breast cancer, and neonatology. I also led the development of an invasive vessel avoidance system for spinal surgery, an endoscopic hypoxia-detecting nerve root retractor for spinal surgery, and an implantable anastomotic coupler for microvascular surgery.


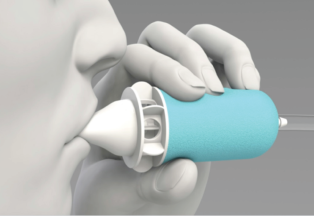
In 2011, I became Sr. VP, Chief R&D and Engineering Officer at Cardiox Corporation where I led the development of the Anazen cardiac shunt detection system and the Anazen liver function monitoring system. These are non-invasive systems consisting of a touchscreen driven console and a set of laser-based fluorescence ear sensors to measure changes in concentration of an injected fluorescent dye. An automated valsalva manuever mouthpiece was also developed to open the shunt, when present, at the desired time. Applications include detection of cardiac shunts (such as patent foramen ovale and atrial septal defects) and liver function monitoring (based on the measured plasma disappearance rate of Indocyanine Green dye).


I believe that the world of
medical devices is just in its infancy, and thanks to recent advances in
microminiaturization, wearable technology, computing, mobile wireless, and
information sharing, we will witness a new century of amazing innovation.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}